Polycystic Ovarian Syndrome and Polycystic Ovaries
Polycystic Ovarian Syndrome (PCOS) and Polycystic Ovaries
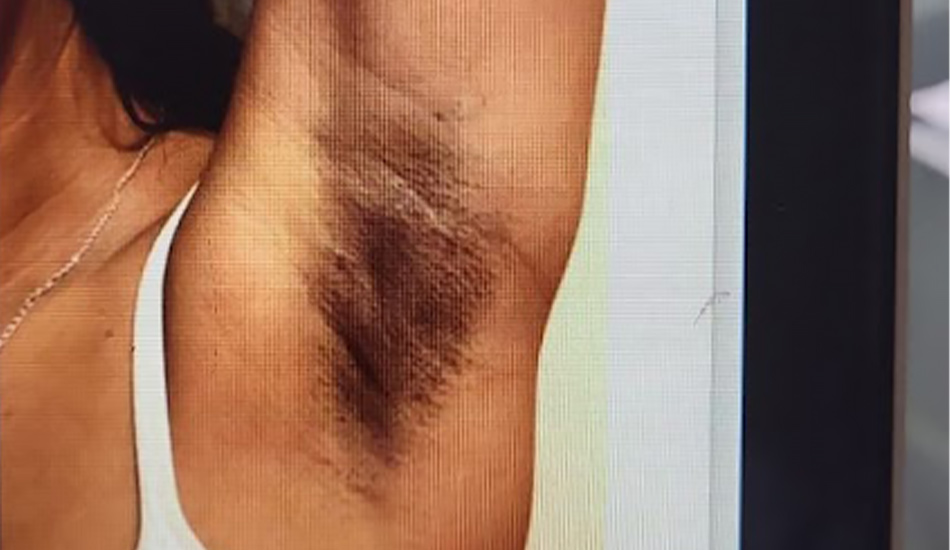
Polycystic Ovarian Syndrome (PCOS) is a very common hormonal disturbance. In my clinical experience, the majority of patient’s concerns are about menstrual cycle changes (irregular or absent periods), infertility issues and skin problems (acne and hirsutism the unwanted hair growth on the face or body) and Acanthosis nigricans, deep pigmentation on the neck and in the armpits). Some women have irregular periods from the onset of menstruation.
Not all patient’s experience the full spectrum of PCOS symptoms, and these will change over the years. Weight gain is a significant problem, and many patients despite dieting, are unable to control their body weight. This increases the risk of infertility.
Approximately 25-% of the female population have polycystic ovaries, but still menstruate and ovulate. A smaller percentage 10-15% will have some of the signs and symptoms although a smaller proportion will have symptoms of the polycystic ovary syndrome-up to 15% of women.
Polycystic ovaries affect up to 25% of them female population.
PCOS is less common and affects 10-15%.
Irregular periods often from the onset of menstruation.
The ovary has 2 purposes: the production of female sex hormones, oestrogen and progesterone and the male hormone testosterone, and also the release of a monthly egg. Once a woman reaches puberty, and starts to menstruate, she will then become fertile and ovulate. We know that ovaries will contain many thousands of eggs which are present in the fetus.
Polycystic ovaries as the name implies will consist of many small follicles, which each contain an egg and may have started to grow but stall, and the ultrasound appearances will confirm that they remain small at a size of about 2-9 mm in diameter.
A polycystic ovary on ultrasound will normally consist of 12 small follicles or cysts. The ovaries tend to be bigger than in women with normal ovaries. I use the Anti-Mullerian hormone blood test as one of the markers for PCOS, and Testosterone as this hormone is usually elevated. I will assess the risks of Diabetes and Adrenal dysfunction.
What are the clinical features of polycystic ovarian syndrome?
Signs or symptoms of high male hormones androgens (hirsutism, alopecia and thinning of hair from the head.)
Acne occurs in association with raised testosterone levels.
Irregular or absent menstrual periods after other causes for this have been excluded.
Polycystic ovaries detected on ultrasound scan.
What causes polycystic ovaries?
A gain in body weight is often a precipitating cause for the development of PCOS symptoms.
Familial tendency.
More common in women from South Asia.
Southern Asian women have disturbed insulin metabolism, and this increases the risk of PCOS.
A family history of Diabetes Mellitus.
Metabolic syndrome.
A high BMI, overweight.
Treatment for polycystic ovarian syndrome?
Menstrual problems Women are disturbed by both irregular and unpredictable nature of their periods. They often tell me how upset they become over experiencing scant periods. For these patients who do not want to conceive, I offer a low dose combined oral contraceptive pill, which also will protect the ovary from premature ageing.
For women who cannot take the pill, and require alternative hormonal therapy to induce regular periods, I offer the progesterone coil (Mirena Intrauterine System) which releases the hormone progesterone into the womb.
Infertility and irregular periods Unfortunately, ovulation is often irregular in PCOS and therefore it will take a longer length of time to conceive. I will therefore arrange the appropriate tests including tracking scans and blood tests to determine the treatment you will need to ovulate, and therefore have a better chance of conceiving. I use not only Clomiphene, but also Metformin.
Acne and related skin problems (caused by high androgen levels) The combined oral contraceptive pill will not only regulate the menstrual cycle, but will treat acne and unwanted hair growth. The combined oral contraceptive pill Dianette contains the “anti-androgen” Cyproterone acetate, and Yasmin has Drospirenone which are particularly effective in reducing unwanted hair. They can help improve hair loss. Spironolactone is also effective in treating both acne and hair loss.
Obesity, Polycystic Ovary Syndrome, and weight loss. A potential treatment for infertility using GLP-1 Receptor Agonists (semiglutide and wegovy)
Obesity in western society has tripled over the last 40 years, and we know that more than 1.9 billion adults were estimated as overweight in 2016, of whom over 650 million were obese.
Obesity is now one of the leading causes of premature death.
41 million children under the age of 5 and over 340 million children and adolescents were estimated to be overweight or obese in 2016.
Obesity will shorten the life and health expectancy of the current generation of children in comparison with earlier generations.
It also will result in PCOS and infertility.
Perhaps using GLP-1 Receptor Agonists (semiglutide) provide a new treatment to improve reproductive health, and long term health.
The scientific literature has demonstrated that obesity is responsible for not onlydifficulty in becoming pregnant, but also long-term infertility. Many scientific publications have confirmed that obese women have poorer reproductive outcomes regardless of the mode of conception. They also are at higher risk of poor pregnancy outcome.
A higher body mass index (BMI) (being overweight) is directly associated with poor fertility outcomes. Polycystic ovary syndrome (PCOS) is one of the leading causes of infertility, and many women with PCOS are characteristically overweight or obese.
There is now a potential role for the glucagon-like peptide-1 (GLP-1) receptor agonists (GLP-1 Ras semiglutide, liraglutide), as potential treatments for obese women with PCOS, who want to conceive.
I currently prescribe metformin as a treatment for PCOS, and it can result in a a 5kg weight loss. This improves the fertility rate, and pregnancy outcome. It improves ovulation, and lowers testosterone.
Clinical researchers have now begun to assess the administration of GLP-1 RA (mainly liraglutide) alone or in combination with metformin in women with obesity and PCOS. Several studies demonstrated significant weight loss and testosterone reduction, but with mixed results relative to improvements in insulin resistance parameters and menstrual patterns.
However, it is clear now that he weight loss effects of GLP-1 RA offer a unique opportunity to expand the treatment options available to PCOS patients.
Weight reduction treatment in women with PCOS or infertility
Weight reduction has demonstrated that there is a clear benefit for women who want to conceive. The existing literature on the effect of weight loss in obese women desiring conception has shown that ovulation was restored in 90% of women and 78% went on to conceive. Weight loss is a vital part of infertility treatment. Weight loss also improved IVF cycle outcomes.
Liraglutide in PCOS
There have now been a series of scientific studies which have shown that short-term treatment with liraglutide either as sole treatment or with metformin, will produce significant weight loss, and improve metabolic function in women who are either overweight or are obese with PCOS.
Summary
The weight loss effects of liraglutide offers Gynaecologists wider treatment options available for women with PCOS.
Weight loss will not only improve fertility outcomes but also reduces the risk of pregnancy complications.
Polycystic ovarian syndrome and polycystic ovaries FAQ's
What can I do to reduce my symptoms from PCOS?
Loose weight, consider a full diabetic screen, increase exercise, and see a dietician.
What is the most effective way to treat PCOS if I do not want to get pregnant?
The combined oral contraceptive pill.
What medical treatments are there for the increased hairiness in PCOS?
The combined oral contraceptive pill, and for weight loss, Metformin.
Can surgery improve ovulation
The good news is that the established technique of ovarian drilling improves ovulation rates and conception rates.
Book an Appointment
Requesting an appointment is easy, Just fill out our form and Mr. Morris’s PA will be in touch within 24 Hours.